Most conversations about healthcare AI companies start with the technology. This one starts with you.
Whether you are a hospital administrator trying to reduce operational costs, a clinical director evaluating tools to support your care teams, or an executive trying to understand where this market is actually heading, the question is the same: what is real, what is working, and how do you make the right call for your organization?
This guide walks through the healthcare AI landscape the way a smart buyer should: understand the market first, evaluate what matters second, and make decisions armed with real clinical and financial evidence.
What Is Actually Happening in Healthcare AI Right Now?
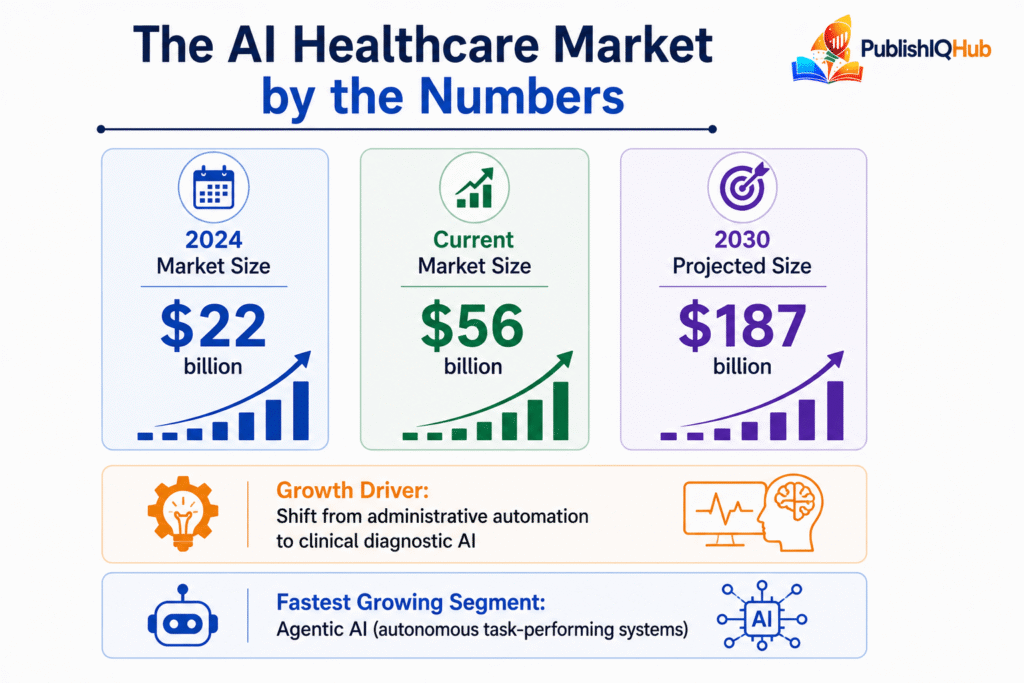
The global healthcare AI market sits at $56.01 billion today and is projected to hit $187 billion by 2030. But the number that matters more than market size is this: the technology has fundamentally changed what it does.
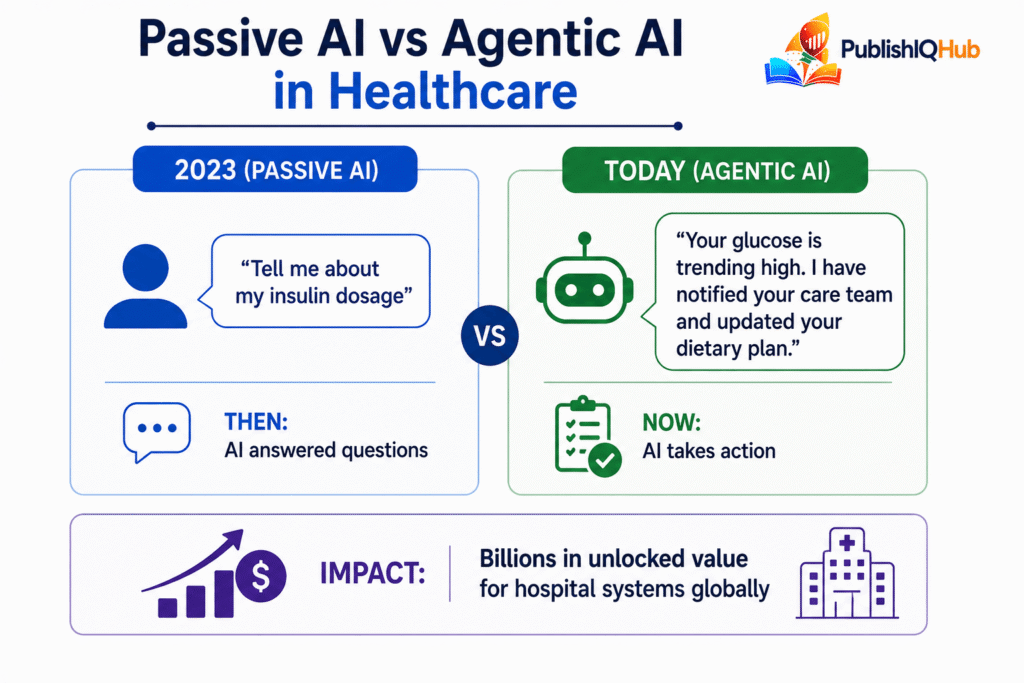
For years, AI in healthcare meant dashboards, flags, and alerts. A radiologist still read the scan. A billing team still filed the claim. A nurse still made the follow-up call. AI sat alongside the workflow and occasionally nudged it. That era is over.
What has replaced it is agentic AI: systems that do not just surface information but take autonomous action. They schedule the follow-up. They file and correct the claim. They alert the care team before the patient even feels sick. This shift is not a product update. It is a category change, and it is the reason investment, adoption, and regulatory scrutiny are all accelerating at the same time.
What Problems Are Healthcare AI Companies Actually Solving?
Before evaluating any vendor, it helps to understand which pain points the industry has organized itself around. There are five that have attracted the most serious investment and the most validated outcomes.
Clinical Documentation Overload
Physicians spend two to three hours documenting for every hour of direct patient care. That ratio is not a workflow inefficiency. It is a systemic crisis driving burnout, reducing time with patients, and degrading the quality of clinical notes that downstream care decisions depend on. Ambient AI documentation has emerged as the highest-adoption category in clinical AI precisely because it attacks this problem without requiring clinicians to change how they work.
Delayed Diagnosis in Time-Critical Conditions
In stroke care, every minute of delayed treatment costs approximately 1.9 million neurons. In pulmonary embolism, delayed detection directly increases mortality risk. AI triage systems in radiology have demonstrated the ability to cut detection-to-notification time by over 80%, with outcomes data that is now published, peer-reviewed, and replicable across health systems.
Revenue Cycle Inefficiency
Insurance denial rates have climbed steadily for years. The administrative costs of managing claims, appeals, and resubmissions now consume a meaningful share of every dollar collected. AI that identifies the specific documentation gaps most likely to trigger a denial, before the claim is ever submitted, is generating some of the clearest and most immediate financial returns in the entire category.
Chronic Disease Management at Scale
There are not enough nurses and care coordinators to follow up consistently with every discharged patient, every patient managing a complex chronic condition, every post-surgical case. AI agents are filling that gap by handling routine touchpoints autonomously and escalating only when something clinically significant surfaces.
Drug Discovery Timelines
AI-native platforms are compressing development timelines by generating and evaluating molecular candidates computationally before a single physical experiment is run, cutting development time roughly in half for organizations that have adopted it at scale. What traditionally took over a decade and more than a billion dollars per molecule is being fundamentally rethought.
Who Are the 15 Medical AI Companies Leading This Market?
| Company | Core Focus | Key Technology | Headline Outcome |
| Tempus | Precision Medicine | Multimodal Models | Drug response prediction (648 genes) |
| Aidoc | Radiology | aiOS Platform | Instant triage for stroke, PE, hemorrhage |
| Abridge | Clinical Documentation | NLP & Ambient AI | Real-time notes (28+ languages) |
| Hippocratic AI | Patient Engagement | Medical LLMs | Virtual nursing automation |
| Viz.ai | Neurovascular Care | Care Coordination AI | 44% faster stroke transfers |
| PathAI | Pathology | Deep Learning | Biomarker discovery |
| Overjet | Dental AI | Computer Vision | Standardized X-ray analysis |
| Insilico Medicine | Drug Discovery | Generative Biology | AI-designed drugs in trials |
| Biofourmis | Hospital-at-Home | Predictive Analytics | 14-day early decline detection |
| Recursion | Biotech Research | Phenomics | Drug discovery mapping |
| Waystar | Revenue Cycle | Predictive RCM | Billing automation at scale |
| Butterfly Network | Imaging | AI Ultrasound | Bedside diagnostics |
| Enlitic | Data Integrity | Metadata AI | Coding accuracy improvement |
| Clarium | Supply Chain | Predictive Modeling | Autonomous disruption resolution |
| Babylon (V3) | Virtual Care | Conversational AI | 10M+ users served |
How Should You Actually Evaluate AI in Healthcare Companies?
The healthcare AI vendor landscape includes billion-dollar enterprises and early-stage startups often making nearly identical claims. Separating genuine clinical value from well-funded marketing comes down to a disciplined evaluation process, not just a feature comparison.
Evaluating Demos Instead of Deployments
A product can look extraordinary in a controlled environment and struggle in a live EHR with real data inconsistencies, real clinician behavior, and real integration constraints. Always ask for reference sites in comparable clinical environments, not curated case studies, and speak to those sites directly.
Measuring the Wrong Outcomes
A documentation tool that saves 40 minutes per shift but introduces new review errors is not a net positive. A triage tool that detects findings faster but generates enough false positives that clinicians start ignoring alerts has made the clinical environment worse. Define your success metrics before evaluation begins, not after the contract is signed.
Underweighting Integration Depth
This is the single most common reason healthcare AI deployments fail to scale. A tool that requires clinicians to leave their EHR, open a separate application, or complete an additional step at the point of care will see adoption collapse within weeks of launch. Workflow integration is not a feature. It is the product.
What Are the Real Risks Every Buyer Needs to Pressure-Test?
The industry has matured past the point where these can be treated as theoretical concerns. Every serious AI in healthcare companies evaluation process should include direct, documented answers to all three.
| Challenge | What It Means for Buyers | What Actually Happens in Reality | Hidden Risk | How Smart Companies Solve It |
| Algorithmic Drift | Model accuracy drops over time | Performance degrades silently until outcomes worsen | Hospitals often don’t monitor continuously | Real-time monitoring + auto-retraining + SLA-based alerts |
| Deskilling Risk | Clinicians rely too much on AI | Skills degrade slowly, not immediately visible | Becomes critical during system downtime | AI-assisted workflows (not AI-led), periodic manual validation |
| Explainability Gap | AI decisions are not transparent | Clinicians ignore outputs they don’t trust | High-performing models still fail adoption | Visual explanations, traceable reasoning, audit logs |
Is Healthcare AI Making Care More or Less Equitable?
This question belongs in every evaluation process, and most buyers are not asking it nearly early enough. Medical AI companies that treat equity as a compliance checkbox rather than a design requirement create real risk: regulatory exposure, performance failures in underserved populations, and reputational consequences that are increasingly difficult to manage.
Why the Equity Problem Exists
AI models perform best on populations that were well represented in their training data. Large academic medical centers have historically generated the most structured clinical data, and models trained on that data may perform less accurately in community hospitals, rural settings, and patient populations with different demographic profiles, disease presentations, and care-seeking behaviors.
Where Buyers Should Specifically Probe
Equity in healthcare AI is often discussed as a compliance requirement, but in practice, it is a performance issue. Systems that are not designed for diverse patient populations do not just create ethical concerns- they deliver inconsistent clinical outcomes.
- Training data bias is the most foundational risk. Most AI models are trained on data from large, well-funded health systems, which tend to represent a narrower patient demographic. In real-world deployments, this shows up as uneven performance—models that work well for some populations but underperform for others. The business and clinical impact is significant: increased risk, reduced trust, and potential regulatory scrutiny. Leading companies are addressing this by diversifying training datasets and, more importantly, publishing performance metrics across different patient subgroups rather than relying on aggregate accuracy claims.
- Access asymmetry is a structural issue rather than a technical one. Advanced AI tools are often deployed first in large urban hospitals with the budget and infrastructure to support them. This creates a widening gap between high-resource and low-resource healthcare environments. In practice, it means that the benefits of AI—faster diagnosis, better monitoring, improved outcomes—are not evenly distributed. Companies that are solving this are rethinking delivery models entirely, moving toward cloud-based deployments, modular pricing, and infrastructure-light solutions that smaller hospitals can realistically adopt.
- Language and literacy gaps are frequently underestimated but have a direct impact on patient outcomes. Many AI systems assume English fluency and a certain level of health literacy, which does not reflect real-world patient populations. This leads to lower engagement, misunderstandings of care instructions, and, ultimately, reduced effectiveness of the tool. More mature solutions are addressing this through multilingual support, voice-based interfaces, and simplified outputs designed for patient comprehension rather than clinical precision alone.
The broader pattern is clear: equity is not a separate layer that can be added after the product is built. It has to be designed into the system from the start. The companies that treat it as a core requirement are not just reducing risk- they are building systems that perform better across the board.
What Does a Good Healthcare AI Decision Actually Look Like?
By the time you reach a vendor decision, you should have already eliminated tools that failed on workflow integration, could not produce real-world clinical evidence in comparable settings, or gave evasive answers on equity and explainability. What remains is a shorter list evaluated against your specific operational context, existing infrastructure, and clinical priorities.
The decisions that go wrong at this stage almost always share a common pattern: the buyer optimized for the most impressive capability rather than the best fit. A tool that can do more things but integrates poorly will consistently underperform a tool that does fewer things and disappears seamlessly into the workflow your clinicians already use.
How Do You Structure the Final Evaluation?
- Match the Tool to a Specific Measurable Problem First
The organizations seeing the strongest returns from healthcare AI are not the ones deploying the most tools. They are the ones that identified a specific, quantifiable problem and evaluated AI against its ability to solve that problem with evidence. Every successful deployment starts with a defined baseline and a defined success metric.
- Require Reference Site Conversations, Not Case Studies
Marketing case studies are written to persuade. Reference site conversations reveal implementation challenges, adoption curve realities, edge cases, and ongoing maintenance requirements that case studies do not include. Ask specifically to speak with clinical end users at reference sites, not just IT or administrative contacts.
- Evaluate the Vendor Relationship, Not Just the Product
Healthcare AI is not a software purchase with a fixed scope. Models need retraining. Regulations change. Clinical workflows evolve. The quality of the vendor’s ongoing support, their responsiveness to performance issues, and their roadmap alignment with your organization’s direction matter as much as the initial product capability.
- Run a Time-Limited Pilot with Real Success Metrics
Before a full contract commitment, negotiate a structured pilot in a defined clinical area with agreed measurement criteria. A vendor who resists a structured pilot with defined success metrics is a vendor who is not confident their product will perform in your environment.
The Vendor Evaluation Framework
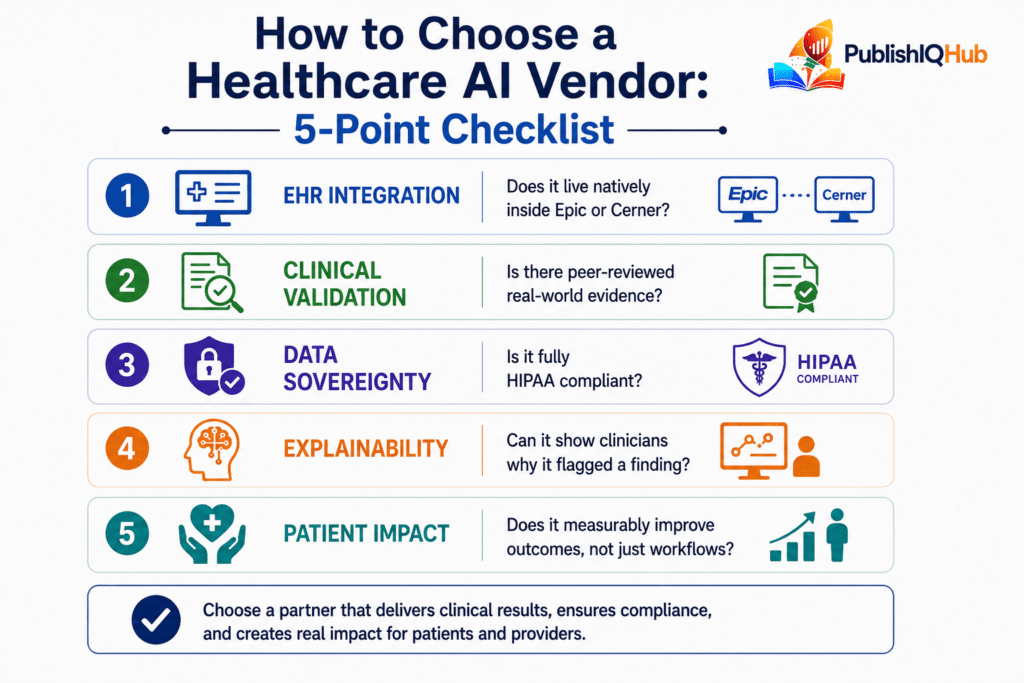
EHR Integration
What to ask: Does it work inside your existing systems without requiring a separate login or workflow?
What it actually tests: Whether the tool fits into real clinical workflows or forces behavior change.
Common mistake buyers make: Treating integration as a “nice-to-have feature” instead of a core requirement.
What best-in-class vendors do: Build deep, native integrations (e.g., directly embedded into systems like Epic Systems), ensuring clinicians never leave their primary workflow.
Clinical Validation
What to ask: Is there peer-reviewed evidence from real-world deployments?
What it actually tests: Whether the tool performs reliably outside controlled demo environments.
Common mistake buyers make: Relying on pilot results or internal vendor studies.
What best-in-class vendors do: Provide multi-site, peer-reviewed validation with real clinical outcome data.
Data Sovereignty
What to ask: Is data handling fully compliant with regulations (e.g., HIPAA) with no ambiguity?
What it actually tests: Legal, operational, and reputational risk tied to data usage.
Common mistake buyers make: Overlooking how data is stored, shared, or reused post-deployment.
What best-in-class vendors do: Offer complete transparency, strong governance frameworks, and audit trails for all data interactions.
Explainability
What to ask: Can clinicians clearly understand why the system made a recommendation?
What it actually tests: Trust, adoption, and clinical usability.
Common mistake buyers make: Accepting high accuracy without understanding decision logic.
What best-in-class vendors do: Provide clinician-readable explanations, traceable reasoning, and visual evidence (not just scores or flags).
Ongoing Support
What to ask: What happens after deployment in terms of model updates and performance monitoring?
What it actually tests: Long-term reliability and sustainability of the solution.
Common mistake buyers make: Treating AI like static software that doesn’t evolve.
What best-in-class vendors do: Offer continuous optimization, retraining cycles, and dedicated support teams to ensure performance improves over time.
Conclusion
The organizations seeing the strongest results from healthcare AI are not the ones that moved fastest. They are the ones who asked the right questions before they moved, matched the technology to a specific measurable problem, and chose vendors whose tools fit the workflow rather than demanding the workflow fit the tool. That discipline, applied consistently, is what separates a transformative AI deployment from an expensive pilot that never scales.
Frequently Asked Questions About Healthcare AI Companies
What do healthcare AI companies actually do?
They build software that uses machine learning to support clinical decisions, automate administrative tasks, accelerate drug discovery, and improve patient monitoring. The category spans radiology triage, ambient documentation, autonomous billing, virtual nursing agents, and AI-powered drug discovery platforms
Which AI in healthcare companies are FDA-cleared?
Aidoc (multiple indications), Viz.ai (stroke and PE), Butterfly Network, and Overjet all hold FDA clearances or approvals. FDA clearance is increasingly a baseline expectation for any tool used in direct clinical decision support, and buyers should treat its absence as a meaningful risk factor for clinical AI tools specifically.
What is the difference between medical AI companies and general AI companies in healthcare?
Medical AI companies build models trained specifically on clinical data, validated against peer-reviewed outcomes, and designed with regulatory compliance as a foundational requirement. General AI companies adapt existing models for healthcare use cases, typically without the clinical validation or safety architecture that the setting demands.
Are AI healthcare startups replacing physicians?
No. Every leading deployment in this space is explicitly built around augmenting physician judgment rather than replacing it. The human-in-the-loop architecture is not just an ethical position. It is a regulatory and clinical requirement that the most mature vendors have embedded into their core product design.
Can healthcare AI reduce disparities in care access?
Yes, when designed with equity as a core requirement rather than a compliance checkbox. Multilingual documentation, point-of-care diagnostics, and virtual care agents are already extending quality care to underserved populations. But poorly designed AI trained on non-representative data can reinforce existing disparities at scale.
What is the single biggest risk when deploying healthcare AI?
Choosing a tool based on demo performance rather than real-world clinical evidence in comparable environments. Algorithmic drift, integration failure, and clinician non-adoption are all downstream consequences of that single upstream mistake.